
En atención a la creciente preocupación sobre la confianza en...
Leer más
How an outbreak became a pandemic: a chronological analysis of crucial junctures and international obligations in the early months of the COVID-19 pandemic
Understanding the spread of SARS-CoV-2, how and when evidence emerged, and the timing of local, national, regional, and global responses is essential to establish how an outbreak became a pandemic and to prepare for future health threats. With that aim, the Independent Panel for Pandemic Preparedness and Response has developed a chronology of events, actions, and recommendations, from December, 2019, when the first cases of COVID-19 were identified in China, to the end of March, 2020, by which time the outbreak had spread extensively worldwide and had been characterised as a pandemic. Datapoints are based on two literature reviews, WHO documents and correspondence, submissions to the Panel, and an expert verification process. The retrospective analysis of the chronology shows a dedicated initial response by WHO and some national governments, but also aspects of the response that could have been quicker, including outbreak notifications under the International Health Regulations (IHR), presumption and confirmation of human-to-human transmission of SARS-CoV-2, declaration of a Public Health Emergency of International Concern, and, most importantly, the public health response of many national governments. The chronology also shows that some countries, largely those with previous experience with similar outbreaks, reacted quickly, even ahead of WHO alerts, and were more successful in initially containing the virus. Mapping actions against IHR obligations, the chronology shows where efficiency and accountability could be improved at local, national, and international levels to more quickly alert and contain health threats in the future. In particular, these improvements include necessary reforms to international law and governance for pandemic preparedness and response, including the IHR and a potential framework convention on pandemic preparedness and response.
Introduction
The COVID-19 pandemic is the result of the rapid international spread of SARS-CoV-2, a coronavirus that causes COVID-19 disease. As of Oct 22, 2021, more than 242·3 million infections and 4·9 million deaths have been documented, making it one of the most extensive pandemics in history,
which occurred despite evaluations showing that many countries were reportedly prepared to respond to an emerging infectious disease.
To understand how SARS-CoV-2 caused a global pandemic and to prepare for future health threats, establishing a clear and accurate understanding of the sequence of key early epidemiological events and of authorities’ responses to the emergence of SARS-CoV-2 is essential. With that aim, the Independent Panel for Pandemic Preparedness and Response (henceforth called the Independent Panel) has developed a chronology of events and actions from December, 2019, when cases were first identified in China, to the end of March, 2020, when COVID-19 cases were found in nearly every country in the world and the outbreak had been characterised as a pandemic. On the basis of these findings, the Independent Panel developed a set of recommendations to improve the speed and efficiency of disease detection and alerts to help countries to respond more effectively to future global health emergencies.
By identifying the timeline of key events, the chronology also enables assessment of adherence to international obligations, in particular, under the International Health Regulations (IHR) 2005, which are currently the only binding international legal instrument dedicated to the prevention, detection, and response to cross-border health threats.
The IHR create obligations for States Parties and set out clear duties and responsibilities for WHO, WHO’s Director-General, and specialised committees in the event of a health threat with potential international consequences.
Using a conceptual framework for key stages from outbreak to pandemic, we map the chronology of documented actions against the obligations under the IHR to establish how systems functioned and to identify potential areas for improvement and further clarity in early outbreak alert and response. From this analysis, we propose a series of corresponding objectives to correct weaknesses in global preparedness for future potential high-impact respiratory pathogens with primary features similar to those of SARS-CoV-2.
These objectives inform and assist in applying the lessons from COVID-19 to reform the IHR and to initiate a potential framework convention on pandemic preparedness and response.
Methods
Three complementary methods were adopted to analyse the timing of events and responses to COVID-19. First, we conducted a systematic review to identify peer-reviewed articles and public reports that examined the scientifically documented origins and the early spread of SARS-CoV-2 (see appendix p 1 for a full overview of search strategy and methodology). Experts, including from China and WHO, were identified to contribute to validation of the findings. Two systematic searches were performed: one on the origins of SARS-CoV-2 and another on the early spread of the virus. The search strategy on the origins was designed to retrieve all eligible articles on the earliest scientific evidence concerning the appearance or spread of SARS-CoV-2, published between Dec 1, 2019, and March 31, 2021, and that met inclusion criteria. The electronic databases MEDLINE, Embase, Global Health, Latin American and Caribbean Center on Health Sciences Information, Western Pacific Region Index Medicus, and Africa Wide Information were searched using the search terms “coronavirus”, “novel virus”, “2019-nCOV”, “COVID-19”, “SARS-CoV-2”, or “Wuhan virus”, following the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines. 6133 articles were identified and a total of 53 publications were included in the final review. The search strategy on early spread was designed to retrieve all eligible articles focusing on the epidemiology of COVID-19 spread published between Dec 1, 2019, and March 31, 2021, in the electronic databases MEDLINE, Embase, Global Health, Latin American and Caribbean Center on Health Sciences Information, Western Pacific Region Index Medicus, and Africa Wide Information. Search terms included “spread”, “transmission”, or “seroprevalence”, and “COVID-19”, “SARS-CoV-2”, “coronavirus”, “novel virus”, or “Wuhan virus”. The results were narrowed to articles that examined, either in real time or retrospectively, the spread of the virus both in China and outside China within the early months of the pandemic (December, 2019, to March, 2020). In both systematic reviews, researchers in relevant fields were contacted to identify additional published and preprint studies. To identify further relevant studies, reference lists of included articles were searched and a forward citation search was performed on included studies using Web of Science. There were no language restrictions in the search strategy. Four authors independently assessed papers for inclusion, extracted data, and assessed the quality of evidence using a metric adapted from the Confidence in the Evidence from Reviews of Qualitative Research approach. A narrative synthesis of the findings was conducted. A meta-analysis was not done because of the substantial methodological heterogeneity in the included studies. 6494 articles were identified in this search, and 57 articles met inclusion criteria for the final review.
Second, as per the Independent Panel’s mandate (appendix p 3), we systematically reviewed internal documents and correspondence from WHO, with a focus on the crucial correspondence that followed the initial detection of the outbreak and activities related to the functioning of the IHR. Specific questions were posed to the WHO Secretariat and responses were provided through a COVID-19 document repository and through discussions with WHO staff members as part of the Independent Panel’s programme of work. In addition, we reviewed 350 technical guidance documents produced by WHO and its Regional Offices and analysed these outputs for their timeliness and evidence base. The timing and nature of key correspondence and guidance documents were mapped onto the chronology.
Finally, to supplement the systematic review, we established an open call for public submissions to share accounts of the timing of the key events during the outbreak. Submissions were then compared and validated against existing public records, with a particular focus on detection, assessment, and reporting activities in line with the IHR.
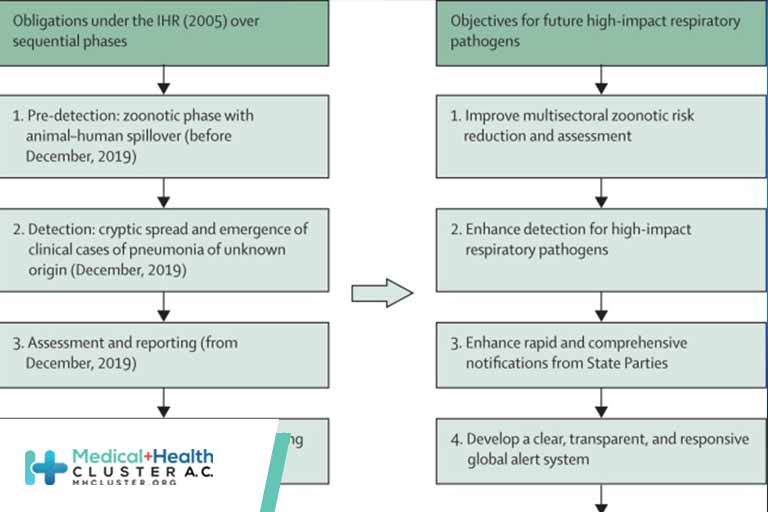
To guide the analysis of the chronology and find areas for improvement for future pandemic preparedness and response, we developed a conceptual framework (figure) for consideration of the steps taken in relation to COVID-19 and associated IHR obligations and potential measures to improve alert in future outbreaks. The relevant IHR provisions include obligations on States Parties to meet minimum core public health capacities, including surveillance, response, and reporting capabilities, assessment and notification of events that might constitute a potential Public Health Emergency of International Concern (PHEIC) within specific timeframes, and ongoing information sharing obligations. The IHR set out the duties and responsibilities of WHO, WHO’s Director-General, and specialised committees, including the power to request verification of reports of events and duties of confidentiality and information sharing, to determine that an event constitutes a PHEIC and to issue temporary recommendations to all States Parties. The IHR also establish the specific criteria for the declaration of a PHEIC. Because the IHR govern country preparedness for potential international health threats and rapid notification and international mobilisation, compliance with these obligations is vital for global health. Establishing how the IHR functioned during the COVID-19 pandemic can inform potential technical, governance, and law reform, including by identifying potential gaps that can guide IHR reform or constitute elements of a new international instrument, such as a pandemic treaty.
Créditos: Comité científico Covid


